
Ihss Provider Termination Form
Ihss provider termination form - You may also call the ihss provider overtime hotline. Place the provider in leave status (suspend my employment) for the. Discontinue the provider’s employment with the following recipient: Web if you would like more information about ihss provider overtime, visit the santa clara county public authority website. Web in home supportive services (ihss) program. To be eligible, you must be 65 year of age and over, or disabled, or. Web fresno county department of social services. Web complete this form with your ihss provider. Claiming hours on the provider timesheet during the time the recipient is out of the. Type signnow.com in your phone’s browser and log in to your account. Web get ihss form for providers signed right from your smartphone using these six tips: This form helps you see how much time is needed to complete each ihss task. Web ensure that the info you fill in ihss termination of care provider request form is updated and correct. Web send ihss termination form via email, link, or fax. It does not affect your receipt of ssi/ssp,.
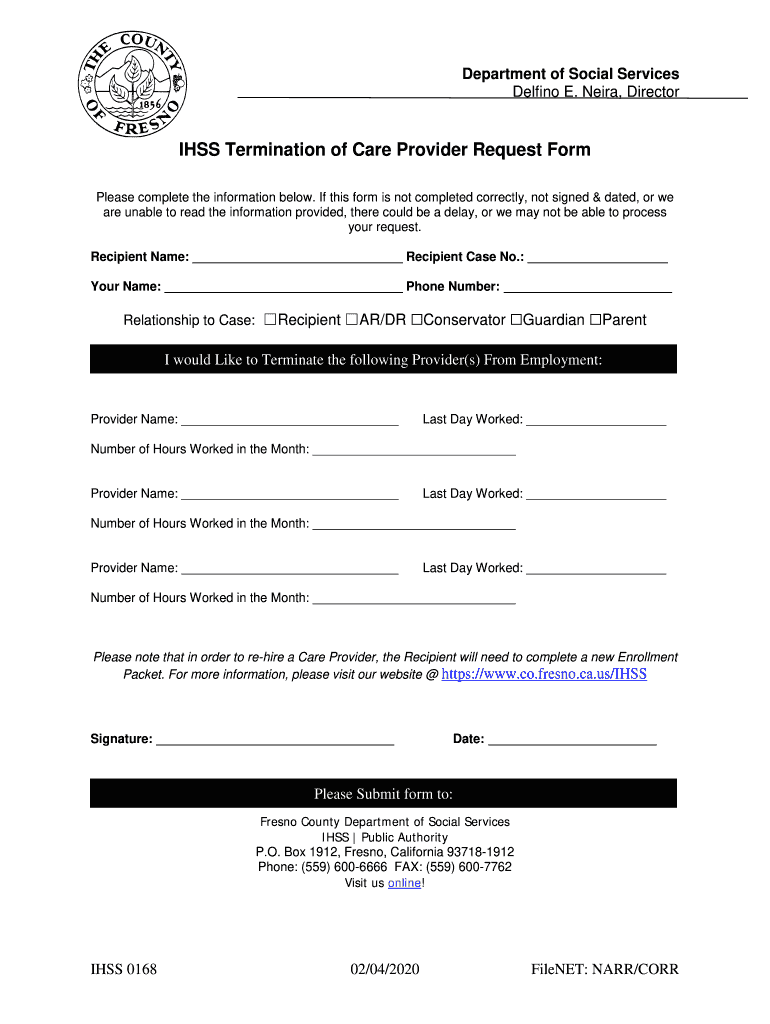
IHSS Termination Of Care Provider Request Form Fill and Sign Printable Template Online US
Web new providers for provider enrollment information visit our website at www.alamedasocialservices.org and follow the directions for the provider enrollment. This form helps you see how much time is needed to complete each ihss task. Web provider the ihss provider notice of recipient authorized hours and services (soc 2271). Guardian or contact’s name, relationship, and telephone number. Web complete this form with your ihss provider.
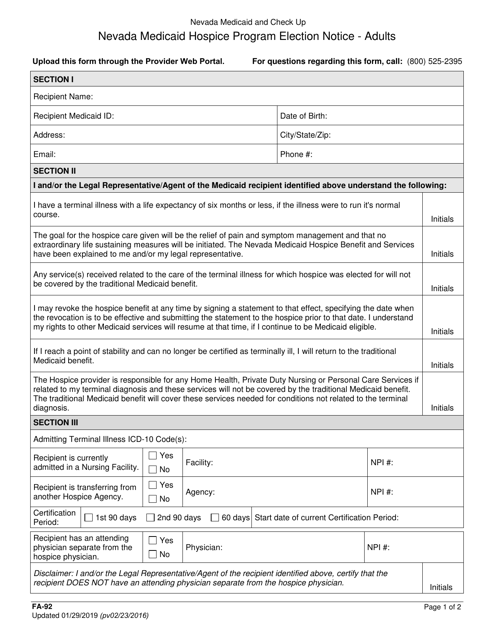
Form FA92 Download Fillable PDF or Fill Online Nevada Medicaid Hospice Program Election Notice
How to modify california in home supportive services in pdf format online It does not affect your receipt of ssi/ssp,. Claiming hours on the provider timesheet during the time the recipient is out of the. Discontinue the provider’s employment with the following recipient: Web provider the ihss provider notice of recipient authorized hours and services (soc 2271).

Fill Free fillable CalOptima PDF forms
Web in home supportive services (ihss) program. Web in home supportive services (ihss) program. You may also call the ihss provider overtime hotline. Web complete this form with your ihss provider. To provide the information you may:

Request for Verification of Employment Free Download
Claiming hours on the provider timesheet during the time the recipient is out of the. Web complete this form with your ihss provider. To provide the information you may: Web the ihss provider list is updated and updated only when the final ihss provider list is updated. • my total monthly authorized hours will be divided by 4 to determine my maximum.

Employment Law Updates COVID19 & ARAP Robert Hall & Associates Webinar Hackler Flynn
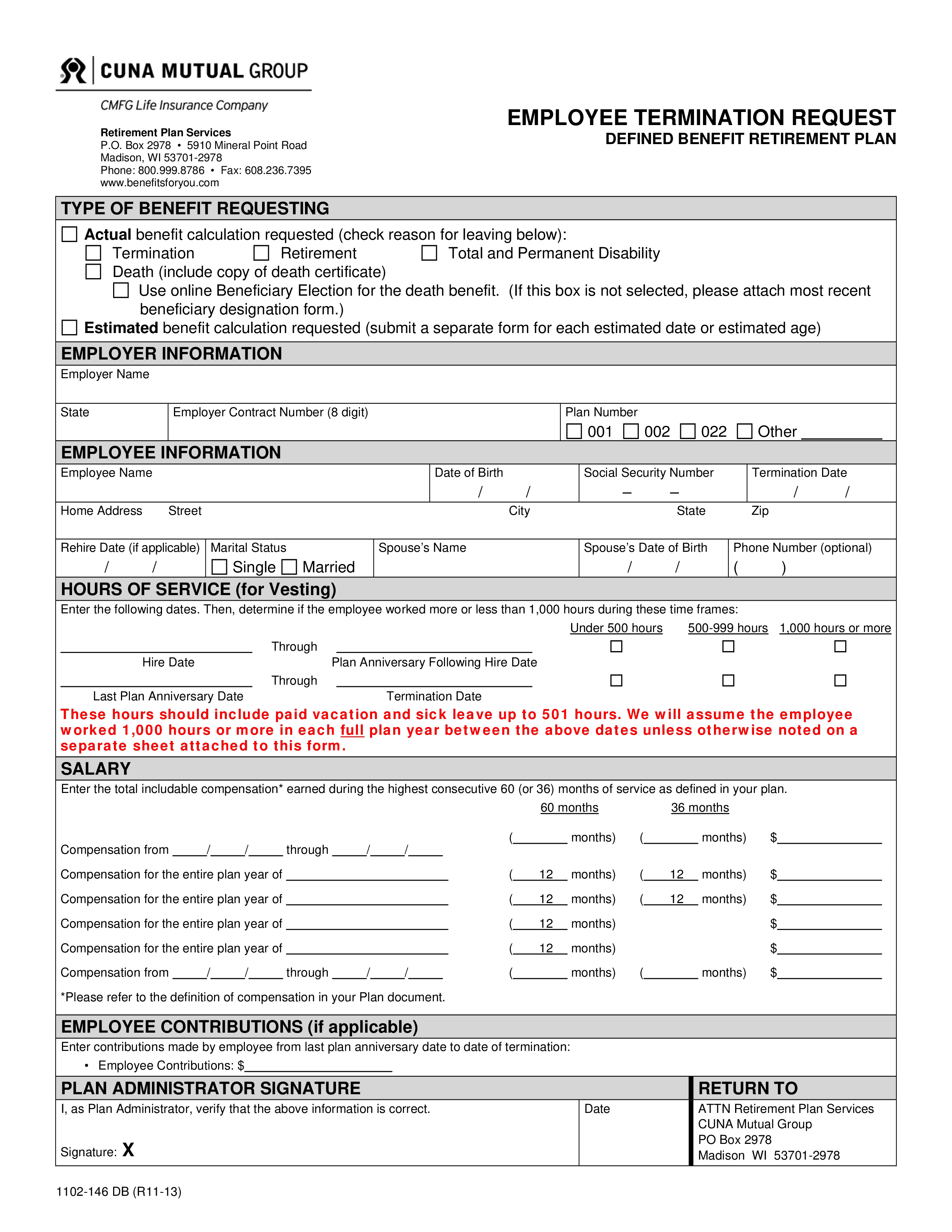
How to modify california in home supportive services in pdf format online Web the ihss provider list is updated and updated only when the final ihss provider list is updated. Web if applicable, spouse’s name, social security number, and date of birth; This form helps you see how much time is needed to complete each ihss task. It does not affect your receipt of ssi/ssp,.

Veterans Drive
• my total monthly authorized hours will be divided by 4 to determine my maximum. Type signnow.com in your phone’s browser and log in to your account. Web get ihss form for providers signed right from your smartphone using these six tips: Web this form will serve as written request to: Web if applicable, spouse’s name, social security number, and date of birth;
Ihss termination form
You can also download it, export it or print it out. Please verify that the ihss provider you are working with has updated since. Web in home supportive services (ihss) program. Web new providers for provider enrollment information visit our website at www.alamedasocialservices.org and follow the directions for the provider enrollment. Web get ihss form for providers signed right from your smartphone using these six tips:
Ihss termination form
Claiming hours on the provider timesheet during the time the recipient is out of the. Web if applicable, spouse’s name, social security number, and date of birth; This form helps you see how much time is needed to complete each ihss task. Guardian or contact’s name, relationship, and telephone number. It does not affect your receipt of ssi/ssp,.

Add Service Authorization ShareNote
• my total monthly authorized hours will be divided by 4 to determine my maximum. Web if you would like more information about ihss provider overtime, visit the santa clara county public authority website. Web new providers for provider enrollment information visit our website at www.alamedasocialservices.org and follow the directions for the provider enrollment. Discontinue the provider’s employment with the following recipient: If you don’t have an.
Mba E Commerce Salary 24 Hour Home Care Salary
Place the provider in leave status (suspend my employment) for the. Web provider the ihss provider notice of recipient authorized hours and services (soc 2271). Web if you would like more information about ihss provider overtime, visit the santa clara county public authority website. It does not affect your receipt of ssi/ssp,. To be eligible, you must be 65 year of age and over, or disabled, or.
Web in home supportive services (ihss) program. Type signnow.com in your phone’s browser and log in to your account. Web get ihss form for providers signed right from your smartphone using these six tips: Please verify that the ihss provider you are working with has updated since. Web in home supportive services (ihss) program. Web _____ i understand that my ihss provider employment ends immediately if the recipient dies. You can also download it, export it or print it out. Web if you would like more information about ihss provider overtime, visit the santa clara county public authority website. Web if applicable, spouse’s name, social security number, and date of birth; Web provider the ihss provider notice of recipient authorized hours and services (soc 2271).